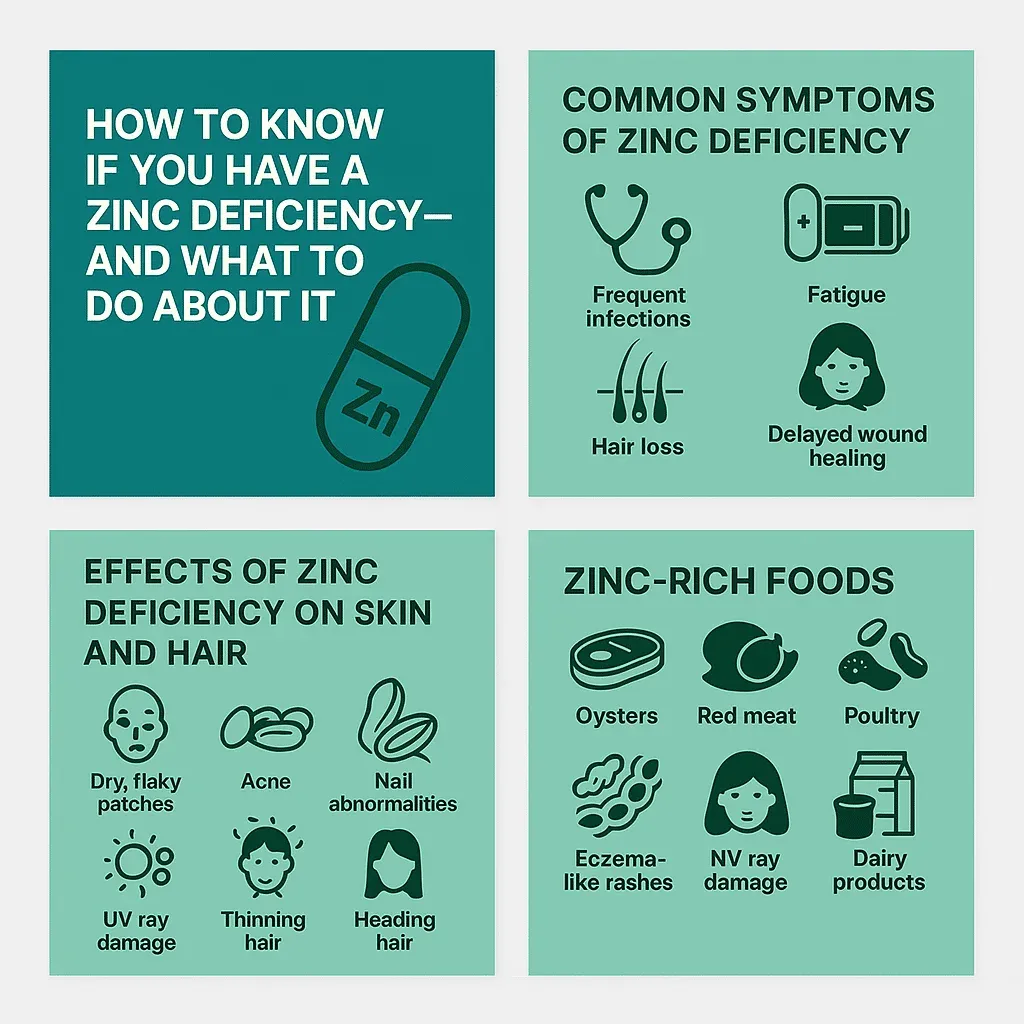
There are nutritional deficiencies that announce themselves loudly — the anaemia that leaves you breathless climbing stairs, the severe vitamin D deficiency that aches in your bones. Zinc deficiency is not like that. It accumulates quietly, degrading function across multiple systems simultaneously, and produces a constellation of symptoms — fatigue, recurrent infections, slow-healing cuts, thinning hair, low mood — that are each easy to attribute to something else. By the time a clinician considers zinc as the culprit, months or years may have passed.
What makes this particularly consequential is the scope of zinc’s role in the body. More than 300 enzymes depend on zinc as a cofactor. It is involved in immune cell production, DNA synthesis, protein manufacture, wound repair, taste and smell perception, hormonal regulation, and cell division. Its absence does not produce a single dramatic failure but a generalised decline across all of these systems simultaneously — which is why the symptoms are so diffuse and so easy to misread.
The global prevalence of zinc deficiency is estimated at approximately 17.3% of the world’s population, according to the International Zinc Nutrition Consultative Group, though some regional estimates run considerably higher. In the Middle East and North Africa, prevalence is estimated at between 20% and 30% among the general population, driven by diets heavy in unleavened bread and legumes that contain high concentrations of phytates — compounds that bind zinc in the gut and significantly reduce its absorption.
For residents of the UAE, several additional factors compound this baseline risk: intense heat that drives meaningful zinc losses through sweat, a large population of vegetarians and vegans for whom plant-based zinc is substantially less bioavailable than animal-derived zinc, and Ramadan fasting patterns that alter eating schedules and zinc intake. Understanding zinc deficiency in the UAE context requires engaging with these specifics rather than relying on guidance written for temperate-climate, omnivorous populations.
What Zinc Actually Does: The Biological Picture
Zinc is a trace mineral, meaning the body requires it in small quantities relative to macronutrients — but the consequences of insufficiency are far from small. Several of its roles deserve specific attention because they explain why the symptoms of deficiency are so wide-ranging.
Immune function. Zinc is required for the development and activation of T-lymphocytes, the white blood cells central to adaptive immune response. It is also involved in natural killer cell function, neutrophil activity, and the production of cytokines — signalling molecules that coordinate the immune response. A zinc-deficient immune system responds more slowly to pathogens and recovers less efficiently from infection. This explains why frequent colds, prolonged illness duration, and slow recovery from minor infections are among the earliest and most consistent symptoms of marginal zinc deficiency.
Wound healing. The skin contains approximately 5% of the body’s total zinc content. Zinc is required at multiple stages of wound repair: inflammation, cell proliferation, re-epithelialisation, and collagen synthesis. Wounds that heal slowly, that are prone to infection, or that leave more prominent scarring than expected are often associated with suboptimal zinc status.
Hormone production. Zinc is essential for the synthesis and metabolism of testosterone, the conversion of thyroid precursors, and insulin function. In men, zinc is concentrated in the prostate and testes, where it supports spermatogenesis and maintains sperm motility and morphology. The link between zinc status and male reproductive health is among the most consistent findings in nutritional endocrinology. Low zinc is associated with reduced testosterone, impaired sperm quality, and reduced libido. In women, zinc supports follicular development, ovulation, and the hormonal regulation of the menstrual cycle.
Skin and hair integrity. Zinc is a cofactor for enzymes involved in keratin production — the structural protein of hair and nails. It also regulates sebaceous gland activity, which influences acne development. Deficiency manifests dermologically as dry or flaking skin, acne that does not respond to topical treatment, delayed wound healing, nail changes including white spots (leukonychia), and hair thinning or shedding.
Taste and smell. Gustin, also known as carbonic anhydrase VI, is a zinc-dependent enzyme produced in saliva that is essential for the development and maintenance of taste buds. Zinc deficiency reduces its production, causing hypogeusia (diminished taste sensitivity) or ageusia (complete loss of taste). Loss of smell (hyposmia) is a related but less consistently documented symptom. These sensory changes are reversible with zinc repletion in most cases.
Cognitive function. Zinc is a modulator of synaptic transmission and is involved in memory formation, learning, and mood regulation through its effects on glutamate and GABA signalling. Low zinc status has been associated with symptoms of depression, irritability, and impaired concentration — though causality in human studies is more difficult to establish than in animal models.y intake crucial—miss a few days and the effects begin to show.
Who Is at Risk: The Groups Most Likely to Be Deficient
Zinc deficiency is not randomly distributed. Several populations face consistently higher risk due to dietary patterns, physiological demands, or medical conditions that increase requirements or impair absorption.
Vegetarians and vegans. This is the single most significant risk category globally, and particularly relevant in the UAE given the large South Asian population, a substantial proportion of whom follow vegetarian or predominantly plant-based diets. The issue is not merely that plant foods contain less zinc than animal foods — though this is true — but that plant foods contain phytates (inositol hexaphosphate), which bind zinc in the gut and inhibit its absorption. Legumes, whole grains, and seeds — the staples of many plant-based diets — are both the primary plant sources of zinc and the highest-phytate foods. The net zinc absorption from a plant-based diet can be 35 to 50% lower than from an omnivorous diet providing the same nominal zinc content. This means vegetarians and vegans may need zinc intakes up to 50% higher than omnivores to achieve equivalent status.
People who sweat heavily. Zinc is lost in sweat at a rate of approximately 0.5 to 1.0 mg per litre, depending on individual variation and acclimatisation status. This is the UAE-specific factor that receives almost no attention in zinc guidance written for general Western audiences. A resident of Dubai who exercises outdoors in summer, or who works in a physically demanding outdoor role during June through September, can lose 1 to 2 litres of sweat per hour during peak heat — representing potential zinc losses of 1 to 2 mg per hour of intense activity. Against a recommended dietary intake of 8 to 11 mg per day for adults, this is a physiologically meaningful loss that must be compensated by dietary intake. UAE residents who exercise regularly, work outdoors, or simply perspire heavily in the climate are at meaningfully higher risk of deficiency than sedentary residents of temperate climates.
People who observe Ramadan fasting. The timing and pattern of food intake during Ramadan — one or two concentrated eating periods in the evening rather than spread across the day — can affect zinc absorption and status. Studies examining zinc levels in populations observing Ramadan fasting have produced mixed results, but the dietary shift toward larger, later meals concentrated around iftar and suhoor can alter the bioavailability of zinc if high-phytate foods dominate those meals. Muslims in the UAE who observe Ramadan fasting and who also have other risk factors for deficiency should consider having their zinc levels checked following the fasting month.
People with gastrointestinal conditions. Inflammatory bowel disease (Crohn’s disease and ulcerative colitis), coeliac disease, irritable bowel syndrome, and short bowel syndrome all impair zinc absorption through different mechanisms. Chronic diarrhoea — which can be more frequent in the UAE due to foodborne illness in an environment with a large restaurant dining culture — also increases zinc losses. People with any chronic GI condition should treat zinc monitoring as routine rather than optional.
Heavy alcohol consumers. Alcohol interferes with zinc absorption in the small intestine, increases urinary zinc excretion, and damages the liver’s ability to store and release zinc. Chronic high alcohol intake is associated with significantly reduced zinc status even when dietary intake is adequate.
Pregnant and breastfeeding women. Zinc requirements increase substantially during pregnancy (to 11 mg/day) and lactation (to 12 mg/day) to support foetal development and breast milk production. Many prenatal supplements include zinc, but dietary intake should also be assessed — particularly for women following plant-based diets.
Older adults. Zinc absorption efficiency declines with age. Older adults also tend to have lower total food intake, and medications common in this demographic — diuretics, ACE inhibitors, antacids — can further impair zinc status.In children, zinc deficiency can also cause growth delays and weakened immunity.

Recognising the Symptoms: What to Look For
No single symptom is diagnostic of zinc deficiency — all can be produced by other causes. However, the combination of multiple symptoms from the following list, particularly in someone with one or more of the risk factors above, warrants investigation.
Immune system symptoms are typically the earliest to appear and most consistently reported: increased frequency of upper respiratory infections, longer duration of illness once infection occurs, and slower return to full energy following recovery. A person who catches every cold that circulates at their workplace, or who takes two to three weeks to fully recover from what others resolve in a week, may have marginal zinc status affecting immune response.
Skin symptoms include acne that does not respond to standard topical treatments, dry or flaking patches particularly on the face and hands, wounds or cuts that take noticeably longer than expected to heal, and perioral dermatitis — a rash around the mouth that is specifically associated with zinc deficiency.
Hair and nail symptoms include diffuse hair thinning (rather than localised pattern loss, which suggests hormonal or genetic causes), increased hair shedding, and white spots or horizontal ridges (Beau’s lines) on the fingernails. Hair thinning related to zinc deficiency is often gradual and bilateral, affecting the entire scalp rather than specific regions.
Hormonal and reproductive symptoms in men include reduced libido, changes in ejaculatory function, and in cases of significant deficiency, reduced sperm quality detectable on semen analysis. In women, menstrual irregularity and reduced fertility can be associated with zinc status, though these are rarely the sole causative factor.
Sensory symptoms — reduced ability to taste or smell — are among the more specific symptoms, as they relate directly to zinc-dependent enzyme activity. If foods that previously tasted strong or flavourful seem blander than expected, or if sense of smell has diminished without an obvious cause such as nasal congestion or recent illness, zinc status is worth investigating.
Cognitive and mood symptoms — persistent low mood, irritability disproportionate to circumstances, difficulty concentrating — are the least specific of all zinc deficiency symptoms and should not be used in isolation as a reason to supplement zinc. They become meaningful when present alongside other symptoms and confirmed risk factors.

Testing: How to Confirm Deficiency
Self-diagnosis of zinc deficiency based on symptoms alone is unreliable. The symptoms are non-specific, and supplementing zinc without confirmed deficiency carries real risks of its own. Proper testing before supplementation is not optional; it is the correct approach.
Serum plasma zinc (also called plasma zinc concentration) is the standard clinical test. A blood draw is sent to the laboratory, and the result is reported in micromoles per litre (µmol/L) or micrograms per decilitre (µg/dL). The reference range varies slightly between laboratories, but generally: plasma zinc below 10.7 µmol/L (70 µg/dL) indicates deficiency; 10.7 to 17.5 µmol/L is considered normal; above 17.5 µmol/L is elevated.
There are important limitations to acknowledge. Plasma zinc reflects recent intake rather than body stores — it can appear normal even in states of tissue-level deficiency if recent dietary intake has been adequate. Results are also affected by time of day (zinc is lower in the morning), recent infection or inflammation (zinc falls during acute illness regardless of intake), and recent high-carbohydrate meals. For this reason, plasma zinc testing is most useful when done fasting, in the morning, and in the absence of active illness.
Urinary zinc excretion is a complementary test that helps assess whether zinc losses through urine are elevated — useful in people with kidney disease or heavy alcohol use.
Hair mineral analysis is a test offered by various private clinics and marketed to consumers as a way to assess long-term zinc status. The scientific evidence for its reliability is limited. Hair zinc can be affected by hair treatments, cosmetic products, hair colour, and contamination in ways that make results difficult to interpret accurately. It should not be used as the primary diagnostic tool.
The zinc taste test — in which a solution of zinc sulphate is held in the mouth and the patient rates the intensity of taste — is sometimes used in clinical practice as a rapid indicator of zinc status. A person with adequate zinc should perceive the solution as intensely bitter almost immediately; a person with deficiency may perceive little or no taste, or a delayed response. It is a useful screening tool but not sufficiently accurate to replace blood testing.
In the UAE, plasma zinc testing is available through government hospitals, private hospital outpatient clinics, and private diagnostic laboratory chains including Aster, Mediclinic, and similar operators. The test does not require a specialist referral in most cases — a GP can order it during a general health review.
Getting Enough Through Food
The recommended dietary allowance (RDA) for zinc is 11 mg per day for adult men and 8 mg per day for adult women. Pregnant women require 11 mg/day and breastfeeding women 12 mg/day. As noted, vegetarians and vegans should target intakes approximately 50% higher than these figures to compensate for reduced bioavailability.
The most zinc-dense food sources, ranked by content per 100g:
| Food | Zinc per 100g |
|---|---|
| Oysters (wild, cooked) | 60 mg |
| Beef (lean, cooked) | 12.3 mg |
| Pumpkin seeds | 10.3 mg |
| Lamb (cooked) | 6.7 mg |
| Hemp seeds | 9.9 mg |
| Cashews | 5.6 mg |
| Pine nuts | 6.5 mg |
| Lentils (cooked) | 1.3 mg |
| Chickpeas (cooked) | 1.5 mg |
| Fortified breakfast cereals | 3–8 mg (varies by product) |
| Yoghurt (full fat) | 1.0 mg |
| Cheddar cheese | 3.1 mg |
| Eggs (whole) | 1.3 mg |
Oysters are by a substantial margin the richest dietary source — a single serving of six oysters provides approximately 32 mg of highly bioavailable zinc, four times the male RDA. For most people, however, dietary variety across red meat, seeds, nuts, legumes, and dairy provides the most practical route to adequate intake.
For plant-based eaters, the phytate problem can be partially mitigated through preparation techniques that reduce phytate content: soaking and sprouting legumes before cooking, using yeast-leavened bread (where fermentation degrades phytate) rather than unleavened flatbreads, and soaking nuts and seeds in water before consumption all meaningfully improve the bioavailability of zinc from plant sources. Cooking legumes thoroughly also reduces phytate content relative to raw.
Adding a vitamin C source to a meal containing plant-based zinc does not directly improve zinc absorption (unlike iron, where vitamin C is genuinely helpful) — but overall dietary quality, including adequate protein intake, supports zinc absorption generally.
Supplements: When They Are Needed, Which to Take, and What Not to Overdo
When dietary adjustment is insufficient, or when a confirmed deficiency requires faster repletion, supplemental zinc is appropriate. There are several forms and important practical considerations.
Forms of zinc in supplements:
Zinc gluconate, zinc citrate, and zinc picolinate are the most commonly used forms in supplements and the best studied for bioavailability. Zinc picolinate has shown marginally better absorption in some human studies. Zinc oxide — common in cheaper supplements — has significantly lower bioavailability and should generally be avoided when other options are available. Zinc sulphate is well absorbed but can cause nausea and gastric discomfort, particularly when taken on an empty stomach.
Dosing for correction of confirmed deficiency:
Standard supplemental doses for correcting confirmed deficiency range from 15 to 30 mg elemental zinc per day. Higher doses of 40 to 80 mg are sometimes used under medical supervision for more significant deficiencies, but should not be self-prescribed. For general supplementation in people with confirmed marginal status or elevated risk, 15 to 25 mg per day is a typical range.
The upper tolerable intake level and why it matters:
The tolerable upper intake level (UL) for zinc in adults is set at 40 mg per day from all sources combined (food plus supplements). Chronically exceeding this level carries real risks, the most significant of which is copper deficiency. Zinc and copper compete for the same intestinal transporters. Long-term high zinc supplementation suppresses copper absorption, and copper deficiency produces its own serious complications: neurological symptoms, anaemia, and immune dysfunction. People who take high-dose zinc supplements for extended periods without monitoring are at genuine risk of inducing copper deficiency while believing they are improving their health.
Acute zinc toxicity from very high doses (150 mg or more in a single dose) causes nausea, vomiting, and gastrointestinal cramps. Chronic intake between 40 and 150 mg per day over months to years causes the copper deficiency risk described above, reduced immune function (counterintuitively, at very high levels zinc suppresses rather than supports immunity), and reduced HDL cholesterol.
What to take zinc with and without:
Zinc absorption is reduced when taken with calcium supplements, iron supplements (relevant for the many women who supplement iron), and foods high in phytates. Ideally, a zinc supplement should be taken between meals or with a low-phytate meal — meat or eggs rather than wholegrain bread or legumes. Taking zinc with a small amount of food (rather than on a completely empty stomach) reduces the nausea that some people experience.
Zinc for specific UAE-relevant scenarios:
People who exercise intensively outdoors in the UAE climate and who are not currently supplementing zinc may benefit from a moderate-dose supplement (15–25 mg/day) during the summer months when sweat losses are highest, provided dietary intake is not already high from animal sources. Vegetarians and vegans in the UAE should discuss zinc status with a healthcare professional and consider routine monitoring at least annually. People observing Ramadan who have existing risk factors for zinc deficiency should have levels tested following the fasting month rather than assuming dietary intake during the eating window is sufficient.

Frequently Asked Questions
How do I know if I have a zinc deficiency without getting tested? The honest answer is that you cannot reliably self-diagnose zinc deficiency from symptoms alone. The symptoms — fatigue, frequent infections, hair thinning, slow wound healing, skin issues — overlap with numerous other conditions and deficiencies. The appropriate first step is a plasma zinc blood test ordered by a GP, which is available at government and private hospitals throughout the UAE. If you have multiple risk factors (plant-based diet, heavy perspiration, GI condition, heavy alcohol intake) and multiple symptoms, the clinical suspicion is stronger — but testing remains the correct course of action before supplementing.
Is zinc deficiency common in the UAE specifically? There are specific reasons why UAE residents face elevated risk relative to general Western populations. Intense heat and humidity drive significant zinc losses through sweat, particularly for people who exercise outdoors or work in physical outdoor roles. The UAE’s large South Asian population includes a substantial vegetarian demographic for whom phytate-heavy diets reduce zinc bioavailability. And Ramadan fasting patterns alter the timing and composition of dietary zinc intake. These factors combine to make zinc status worth routine monitoring for anyone in the UAE with risk factors, even in the absence of obvious symptoms.
Can I just take a zinc supplement without getting tested? Taking a standard-dose supplement (10–15 mg per day) as a general precaution carries minimal risk for most adults, as it is at or below the RDA. However, taking higher doses without confirmed deficiency is inadvisable because of the copper deficiency risk associated with long-term high zinc intake. The upper tolerable limit for zinc is 40 mg/day from all sources. People who take zinc at doses above 25 mg per day for extended periods should monitor both zinc and copper status, ideally through blood testing every six to twelve months.
What is the best form of zinc supplement to take? Zinc picolinate, zinc citrate, and zinc gluconate are the best-studied forms with good bioavailability. Zinc oxide, found in many budget supplements, has significantly lower absorption and is best avoided when alternatives are accessible. All forms are better absorbed when taken between meals or with a low-phytate meal rather than with high-fibre, high-legume meals that contain phytates.
How quickly does zinc supplementation correct a deficiency? Immune function improvements from zinc repletion can begin within two to four weeks of correcting a deficiency. Skin and hair improvements take longer — typically two to four months, as these reflect tissue turnover rates rather than immediate biochemical changes. Taste and smell abnormalities related to zinc deficiency typically begin improving within four to eight weeks. Full repletion and normalisation of plasma zinc levels generally takes eight to twelve weeks of consistent supplementation at appropriate doses.
Does zinc help with hair loss? Zinc deficiency is a reversible cause of diffuse hair thinning and increased shedding. If hair loss is caused by zinc deficiency, correcting the deficiency will halt the shedding and allow regrowth over two to four months. However, zinc supplementation does not improve hair loss that is caused by androgenetic alopecia (pattern baldness), thyroid dysfunction, iron deficiency, or other non-zinc causes. If hair loss is your primary concern, a full panel including zinc, ferritin, thyroid function, and hormones is more informative than zinc testing alone.
Always consult a qualified doctor or registered dietitian before starting zinc supplementation, particularly at doses above 15 mg per day or if you have any existing health condition or are taking medications. The UAE Ministry of Health and Prevention recommends discussing all supplementation with a licensed healthcare provider.